
Comparison the Diagnostic Value of Doppler Ultrasonography to Biopsy, in Evaluation of Post-transplant Complications and Kidney Function
Abstract
Background
Doppler ultrasonography can evaluate vascular and renal parenchymal disorders. In this study, color Doppler patterns in transplanted kidneys were compared with histological diagnosis to develop diagnostic models for transplanted kidney failure.
Method
45 kidney transplant patients participated in this prospective study (16 suffered acute tubular necrosis (ATN), and 29 had transplant rejection). All patients had color-Doppler ultrasonography to measure kidney parameters and Doppler indices. Serum creatinine levels also assessed the transplanted kidney's function.
Result
Ultrasound showed a significant difference between the two groups in iliac and interlobar PSV. The ROC analysis showed a high diagnostic value of the iliac artery PSV, in distinguishing ATN from kidney transplant rejection. Serum creatinine level correlated directly with transplanted kidney volume, renal cortical thickness, and transplanted kidney length, and inversely with interlobar artery PSV and EDV. In graft rejection patients, the only significant inverse correlation was found between serum creatinine level and PSV of the iliac artery and EDV of the intrelobar artery.
Discussion and conclusion
The iliac artery PSV can differentiate between ATN and rejection after renal transplantation. Evaluation of renal metric parameters along with PSV and EDV of the interlobar artery (in patients with ATN) and iliac artery and interlobar artery (in transplant rejection) help determine renal dysfunction.
Article Information
- Received
- Accepted
- Published
Academic Editor: Ian James Martin, Edith Cowan University, USA
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2022 Roja Hajipour, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Seyed Morteza Bagheri, Department of Radiology, School of medicine, Iran University of Medical Sciences —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
Considering the quality of life of transplant patients compared to dialysis patients, the preferred treatment for end-stage renal failure is kidney transplantation. About 69,000 kidney transplants are performed annually in the world 1. In the United States, the one, three, and five-year survival rate of these transplants are 91%, 82%, and 72%, respectively 2. Despite improvements in surgery and new immunosuppressive drugs, many transplants continue to have a variety of complications, including vascular and parenchymal defects 3, 4, 5, 6. For faster identification of these complications, transplant patients are under special assessments, mainly serial assessments of serum creatinine, urine volume, and sonographic parameters 7, 8. Despite the key role of ultrasound in diagnosing vascular complications in transplant patients, the role of this method in determining parenchymal complications of transplant is still unclear. Parenchymal diseases can be classified into immunological, infectious, and drug-induced, which in many cases cause delayed onset of transplant function, prolonged hospital stay, and overall shortening of transplant life 9, 10. Currently, the main role of ultrasound is to rule out other causes of transplant failure, and these parenchymal disorders are usually differentiated after taking biopsy specimens and histological assessments 11, 12. Due to the invasiveness of the biopsy process, its complications, and costs, having a noninvasive alternative such as ultrasound can be beneficial. In this study, by comparing color Doppler patterns in transplanted kidneys and comparing the results with histological diagnosis, an attempt was made to provide diagnostic models based on Doppler ultrasonography parameters to differentiate the causes of transplanted kidney failure.
Materials and Methods
This prospective study was performed on 45 patients undergoing kidney transplantation (16 suffered acute tubular necrosis or ATN, and 29 had transplant rejection). The study period was 2021 to 2022. Inclusion criteria: Any kidney transplant patient with increased creatinine and kidney dysfunction (suspect for ATN or rejection), in the years 2021 to 2022, referred to our hospital (Hasheminejad Hospital, Urology and Kidney Center, Tehran Iran)
Exclusion Criteria
Patients with vessel involvements (arterial thrombosis/ stenosis, or venous thrombosis) were exclude). Because these diseases affect the disease course. Cases with Peri-graft collection cases were also excluded, because they change the wave/ pattern of ultrasound, and cannot be evaluated.
Reviewing patient's hospital files collected the baseline characteristics, including demographics. All patients were assessed by color-Doppler ultrasonography to assess the values of diametric kidney parameters (length and volume of the transplanted kidney and thickness of the renal cortex) and Doppler indices (arterial peak systolic velocity (PSV), end-diastolic velocity (EDV), resistive index (RI), pulsatility index (PI), and renal vein Doppler index. The functional state of the transplanted kidney was also assessed by measuring serum creatinine levels. In total, the biopsy results with sonographic findings in the two groups of patients were examined. In addition to determining the value of each sonographic parameter in the differential diagnosis of these two post-transplant events, we also evaluated the relationship between each parameter and serum creatinine level as an indicator of renal function.
For statistical analysis, results were presented as mean ± standard deviation (SD) for quantitative variables. They were summarized by frequency (percentage) for categorical variables. The ROC curve analysis was considered to determine the value of each parameter to differentiate ATN from rejection. Pearson's correlation test tested the correlation between the variables. The t-test or Mann-Whitney U test compared the quantitative variables. P values of ≤ 0.05 were considered statistically significant. The statistical software SPSS version 23.0 for windows (IBM, Armonk, New York) was used for the statistical analysis.
Results
Regarding pathological evaluation, 16 (35.6%) had ATN, and 29 (64.4%) had transplant rejections. Regarding sex distribution in the ATN and transplant rejection groups, 87.5% and 65.5% were men, respectively, indicating no difference (p = 0.164). The mean age of patients in the two groups was 35.38±9.19 years and 37.69±10.82 years, respectively, with no difference between the two groups (p = 0.474).
Table 1 indicates the difference in sonographic parameters between the two groups suffering ATN and graft rejection. Ultrasound evaluation showed a significant difference between the two groups in terms of PSV of the iliac artery and PSV of interlobar artery. Based on the analysis of the area under the ROC curve, the area under the curve for the PSV of the iliac artery was 0.744 (95% confidence interval equal to 0.593 to 0.888), and for the PSV of the interlobar artery was 0.597 (95% confidence interval equal to 0.424 to 0.770) which indicated the diagnostic value of only the PSV of the iliac artery in differentiating between ATN from transplanted kidney rejection (considering the level below the acceptable curve above 0.70). Accordingly, the best cut-off point for PSV of the iliac artery in differentiating between ATN from graft rejection was 89, yielding a sensitivity of 82.8% and a specificity of 56.2% in differentiating ATN from renal rejection (Figure 1).
Figure 1. The area below the ROC curve for PSV of the iliac and interlubar arteries in the distinction between ATN and transplant rejection groups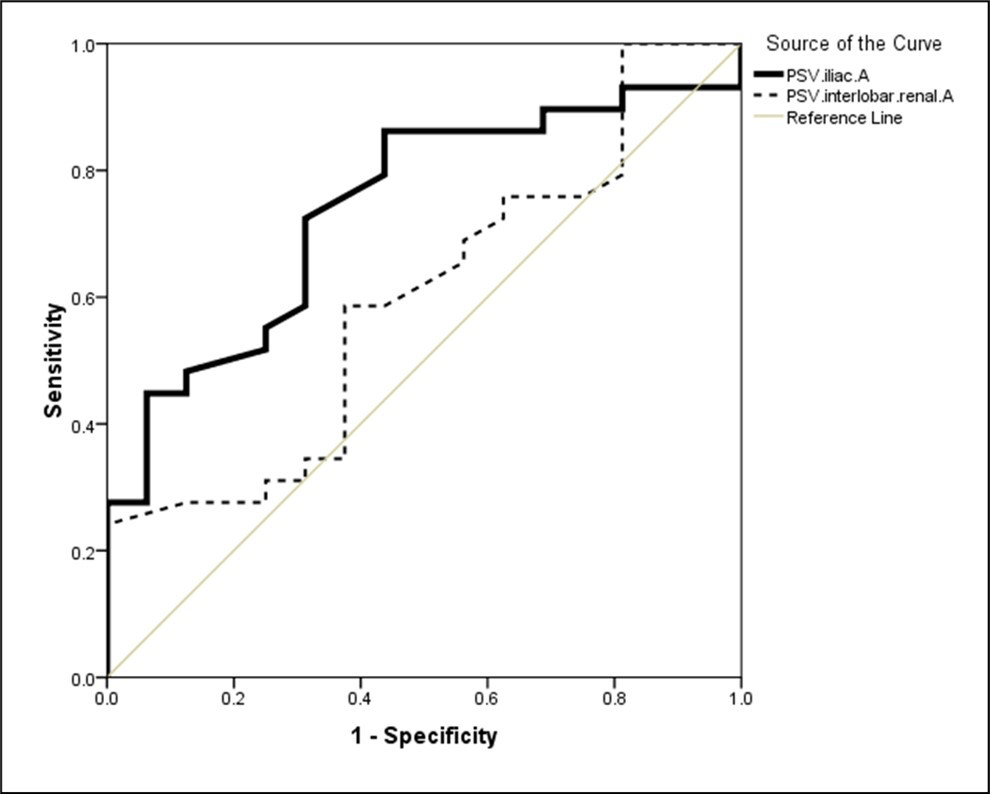
Download figure
Regarding the relationship between serum creatinine level and Doppler indices in patients with ATN (Table 2), there was a significant direct correlation between serum creatinine level with transplanted kidney volume, transplanted renal cortical thickness, and transplanted kidney length, as well as significant inverse correlation with PSV of the interlobar artery and EDV of the interlobar artery. In this group of patients, the correlation between serum creatinine level and other indicators was insignificant. Regarding the relationship between serum creatinine level and Doppler indices in patients suffering graft rejection, the only significant but inverse correlation was found between serum creatinine level and PSV of the iliac artery and EDV of the intrelobar artery (Table 2).
Table 1. Doppler index values in patients under evaluation| Index | Group with ATN | Group with rejection | P value |
| PSV of iliac artery | 88.74±20.98 | 115.66±37.29 | 0.003 |
| PSV of main renal artery | 110.96±38.68 | 125.62±45.64 | 0.253 |
| PSV of interlubar artery | 29.42±11.54 | 40.55±22.91 | 0.036 |
| EDV of interlubar artery | 8.51±3.72 | 11.04±6.90 | 0.116 |
| RI of interlubar artery | 0.74±0.08 | 0.73±0.09 | 0.483 |
| PI of interlubar artery | 1.52±0.61 | 1.61±0.68 | 0.659 |
| Renal venous Doppler | 24.81±6.15 | 22.24±4.34 | 0.182 |
| Volume of kidney | 227.28±69.76 | 190.69±58.84 | 0.086 |
| Cortical thickness | 16.69±1.58 | 15.83±2.70 | 0.185 |
| Length of kidney | 123.38±10.53 | 114.28±10.41 | 0.072 |
| Index | ATN | Rejection | ||
| Correlation coefficient | P value | Correlation coefficient | P value | |
| PSV of iliac artery | -0.215 | 0.424 | -0.375 | 0.045 |
| PSV of main renal artery | -0.104 | 0.702 | -0.142 | 0.464 |
| PSV of interlubar artery | -0.877 | 0.001 | -0.225 | 0.241 |
| EDV of interlubar artery | -0.697 | 0.003 | -0.376 | 0.044 |
| RI of interlubar artery | -0.274 | 0.304 | 0.328 | 0.082 |
| PI of interlubar artery | -0.462 | 0.072 | 0.166 | 0.390 |
| Renal venous Doppler | -0.089 | 0.744 | -0.037 | 0.850 |
| Volume of kidney | 0.668 | 0.005 | -0.036 | 0.853 |
| Cortical thickness | 0.527 | 0.036 | 0.199 | 0.300 |
| Length of kidney | 0.770 | 0.001 | -0.051 | 0.794 |
Discussion
Acute or delayed complications are not due to unexpected kidney transplantation; imaging techniques are the most important tool in evaluating and predicting such complications. Naturally, the use of cheaper, more specific, non-nephrotoxic, as well as portable methods is of paramount importance. In this regard, using Doppler ultrasonography to evaluate vascular and renal parenchymal disorders can be particularly interesting.
Vascular problems account for 5–10% of post-transplant difficulties, but they often induce graft loss. B-mode and Doppler ultrasound are essential in diagnosing renal allograft failure. Doppler ultrasound is extremely specific for transplanted renal artery stenosis, pseudoaneurysms, arteriovenous fistulas, and artery or vein thrombosis. Color Doppler indexes provide great diagnostic accuracy and are especially beneficial during post-transplantation follow-up. Contrast-enhanced ultrasound increases the accuracy of ultrasonography in diagnosing transplanted kidney vascular complications 18
Many recent studies have mentioned the high capability of this tool and its related parameters in predicting the occurrence of complications after kidney transplantation 11, 12, 13, 14, 15. First, the results of the present study showed that in two categories of complications after kidney transplantation, namely ATN and transplant rejection, the parameters obtained from Doppler ultrasonography can be beneficial in distinguishing the two complications from each other. In this regard, it was shown that the PSV parameter of the iliac artery as the most important, most accurate, and sensitive indicator could make such a distinction that values above 89 of this parameter will be more consistent with graft rejection than ATN.
Interestingly, other indices such as RI or PI of the interlobar artery, renal vein Doppler, diametric indices of the transplanted kidney, or even serum creatinine levels were not used to differentiate the two disorders after diagnostic ligation. Therefore, in cases where there is doubt about the distinction between the two complications, the most critical parameter of Doppler ultrasound in their differentiation will be the PSV parameter of the iliac artery. As shown in other studies, there is increase in arterial AI levels and serum creatinine levels in both ATN and transplant rejection lesions. Changes in renal structural parameters are completely non-specific for both phenomena. Therefore, using the PSV parameter of the iliac artery can be very helpful and even prognostic in diagnosing and differentiating these findings.
As a second finding, it was shown that in both groups of patients with ATN and transplant rejection, renal dysfunction based on elevated serum creatinine levels could be predicted using ultrasonic parameters. The correlation between patients' serum creatinine levels with parameters such as PSV of the interlobar artery and EDV of the interlobar artery (for patients with ATN) as well as PSV of the iliac artery and EDV of the interlobar artery (for patients with transplant rejection) indicates the ability of these parameters in advancing renal dysfunction following renal transplantation. In this regard, more emphasis has been placed on the EDV value of interlobar arteries in the early prediction of renal dysfunction. Various studies have discussed the diagnostic value of each ultrasonographic parameter to predict the complications after kidney transplantation, especially transplant rejection. In Sakhaei et al 16 study, the PI parameter is still a predictor of graft rejection. In the study of Elec et a 17, the increase in RI was also an important indicator in the distinction between early and delayed dysfunction.
What is the high advantage of the present study over other studies, firstly, was the study of ultrasonographic parameters in distinguishing between ATN and transplant rejection, which in many cases is one of the most important problems of sonologists and nephrologists. Secondly, in the present study, along with renal metric indices, including kidney length, cortex thickness, and volume, we simultaneously evaluated Doppler parameters. We evaluated the ability of each to predict the occurrence of post-transplant disorders. However, the most important limitation of this study was its small sample size, which may affect the results' significance.
Using a multimodal imaging approach is important, with ultrasound-Doppler as the first-line imaging study. More imaging studies are often needed depending on the clinical situation and the results of the first ultrasound. Renal functional MRI is a growing field that has a lot of potential for finding problems with transplants early on. Multiparametric MRI could be used in clinical practice as a noninvasive "one-stop" modality for early diagnosis and longitudinal monitoring of renal allograft dysfunctions. This is important for guiding the right interventions to delay or stop irreversible kidney damage. With the number of kidney transplants going up quickly and patient survival rates increasing, radiologists need to know the anatomical and functional complications in a transplanted kidney 18.
Limitations of study
The sample sized was small. Although, we tried to include all available cases transplantation during the two years of study
The cause of kidney transplant was not determined in some patients. We did not analyze this part.
Conclusion
The PSV of the iliac artery will have a high value for distinguishing between two complications after renal transplantation, namely ATN and transplant rejection. Evaluation of renal metric parameters along with PSV of the interlobar artery and EDV of the interlobar artery (in patients with ATN) and PSV of the iliac artery and EDV of the interlobar artery (in patients with transplant rejection) are very valuable and useful in predicting renal dysfunction.
References
- 1.Viklicky O, Novotny M, Hruba P. (2020) Future developments in kidney transplantation. , Curr. Opin. Organ Transplant 25, 92-98.
- 2.Garg N, Poggio E D, Mandelbrot D. (2021) The Evaluation of Kidney Function in Living Kidney Donor Candidates. , Kidney 2(9), 1523-1530.
- 3.Alvarado F, Cervantes C E, Crews D C, Blanck J, Al Ammary F et al. (2022) Examining post-donation outcomes in Hispanic/Latinx living kidney donors in the United States: A systematic review. , Am J Transplant
- 4.Reyna-Sepúlveda F, Ponce-Escobedo A, Guevara-Charles A, Escobedo-Villarreal M, Pérez-Rodríguez E et al. (2017) Outcomes and Surgical Complications in Kidney Transplantation. , Int J Organ Transplant Med 8(2), 78-84.
- 5.Mehmet H, Fatih B, Aydıncan A, Mahir K, Ümit O et al. (2016) Surgical Complications After Kidney Transplantation. Exp Clin Transplant. 14(6), 587-595.
- 6.Ammi M, Daligault M, Sayegh J, Abraham P, Papon X et al. (2016) . , Evaluation of the Vascular Surgical Complications of Renal Transplantation. Ann Vasc Surg 33, 23-30.
- 7.Bayashi K, Censullo M L, Rossman L L. (2007) Interventional radiologic management of renal transplant dysfunction: indications, limitations, and technical considerations. , Radiographics 27, 1109.
- 8.Khai Gene Leong, Coombs Peter, Kanellis John. (2015) Renal transplant ultrasound: The nephrologist's perspective. , Australas J Ultrasound Med 18(4), 134-142.
- 9.Datta R, Sandhu M, Saxena A K, Sud K, Minz M et al. (2005) Role of duplex Doppler and power Doppler sonography in transplanted kidneys with acute renal parenchymal dysfunction. Australas Radiol. 49(1), 15-20.
- 10.Irshad A, Ackerman S, Sosnouski D, Anis M, Chavin K et al. (2008) A review of sonographic evaluation of renal transplant complications. Curr Probl Diagn Radiol. 37(2), 67-79.
- 11.Vahedifard F. (2022) Ultrasound-guided intervention for chronic abdominal wall pain; Overlooked but curative approach. J Clin Images Med Case Rep. 3(5), 1836.
- 12.Kim N, Juarez R, Levy A D. (2018) Imaging non-vascular complications of renal transplantation. , Abdom Radiol (NY) 43(10), 2555-2563.
- 13.Granata A, Clementi S, Clementi A, F Di Pietro, Scarfia V R et al. (2012) Parenchymal complications of the transplanted kidney: the role of color-Doppler imaging.G. , Ital Nefrol 29(57), 90-8.
- 14.Tabriz Moradi, H. (2021) . , Survey of Mast Cell Density in Transitional Cell Carcinoma. Iranian Journal of Pathology 16(2), 119-127.
- 15.Sakhaei S, Bakhtavar K, Âkhlaghpour S. (2001) Value of the Doppler sonography in the diagnosis of the rejected Tramsplanted kidneys . , J Mazandaran Univ Med Sci 11(33), 52-56.
- 16.Florin Ioan Elec.Alina Daciana Elec, Sorana Bolboaca, Mihai Adrian Socaciu, Adriana Milena Muntean, Gheorghiță Iacob, Tudor Moisoiu, Răzvan Zaro, Alexandra-Ioana Andries, Maria Ramona Badulescu, Radu Mihai Ignat, Radu Ion Badea. (2020).Contrast-enhanced ultrasonography in the initial evaluation of the kidney graft function: a pilot study. Med Ultrason. 22(3), 272-278.
Cited by (1)
This article has been cited by 1 scholarly work according to:
Citing Articles:
Nauka, novye tehnologii i innovacii Kyrgyzstana. (2024) OpenAlex Crossref Semantic Scholar