
The Heart Physiology in Fertile Female and The Heart Pathophysiology in Post Menopausal Female. The Contribution of Molecular Biology, Maintaining Cardiac Hemodinamy and Electrophysiology
Abstract
Maintaining Cardiac Hemodinamy and Electrophysiology
Author Contributions
Academic Editor: Amal Ibrahim Hassan Ibrahim, Department of Radioisotopes, Nuclear Research Centre, Atomic Energy Authority.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2024 Samuel Sclarosky
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors declare no conflict of interest.
Citation:
Introduction
The physiology of the heart in fertile women and the heart of the female sex in mammals is a masterpiece of evolution over 150 million years. Hormones, after female sexual maturation, prepare the heart to overcome the efforts during pregnancy and childbirth. In female animals, molecular biology does not differ from that of humans. However, during childbirth, animals generally do not have difficulties, given that the shape of the head and the size of the hips (which have a protruding brain, require a great physical effort accompanied by extreme pain in women. This phenomenon appeared when Homo sapiens developed a large forehead (significant growth of the frontal lobes, which occupy 36-38% of the brain size compared to 19% in chimpanzees and 8% in dogs.
Estrogen and collagen in the heart; there are 2 types of collagen in the heart, 1 secreted by the fibroblast, hard collagen (collagen I) that maintains the structure of the heart, and collagen III, soft collagen, which functions to maintain the myocardium's ductility during diastole.2 The ratio between collagen I and III is 1/3, suggesting that under basic conditions, there is more hard collagen than soft in the heart. During pregnancy, the ratio is reversed in favor of collagen III/ 3_. This increase in collagen III allows greater ductility to the left ventricle, increasing diastolic capacity. This diastole increases the cardiac minute volume by a third, without increasing the heart rate 4. A marathon runner needs more than 150 beats per minute to increase his minute volume by a third. It is estimated that the effort of a woman during pregnancy spends the same energy that an Olympic runner would in 18 competitions. Also, estrogen stimulates the fibroblasts to secrete more collagen III in the right atrium. This dilation increases the entry of blood flow, contributing to an increase in cardiac output. 5The physiology of the right atrium's fibroblast is similar to that of the abdominal skin, as it also stretches due to a significant increase in collagen III.
Estrogen and adrenaline
Estrogen has control over the adrenaline secreted from the adrenal medulla and the adrenaline secreted from the sympathetic system.6 This control is of utmost importance during childbirth, given the effort and pain, a large amount of catecholamines are secreted, and stimulating the beta receptors can be very harmful to the integrity of the cardiac muscle.7
Estrogen and calcium metabolism
Calcium levels can vary throughout the month. During the premenstrual period, when there is a decrease in estrogen, there is also a decrease in calcium. In the heart, there is an enzyme, osteopontin, which protects this organ from excessive calcium deposition and directs it towards the bone system8. Estrogen controls cAMP in the entry of calcium channels to the cardiac sarcoplasm (calcium reservoir in the myocyte).9 During systole, calcium enters the myocyte through a physical phenomenon, without the need for energy. During diastole, to release calcium from a low concentration area towards the sarcoplasmic reticulum, a pump, SERCA (Sarcoplasmic Endoplasmic Reticulum Calcium ATPase), 10 and an enzyme, phospholamban, are needed to reinforce it. Both SERCA and the latter are controlled by estrogen.11 Therefore, estrogen has a critical importance in diastolic function and, along with the increase of collagen III during pregnancy, to increase cardiac output.
Estrogen and mitochondria
Mitochondria provide energy to the cardiac muscle. The mitochondrion, with glucose, fatty acids, and oxygen, produces adenosine triphosphate (ATP).12 Through fission, ATP loses a phosphate anion. This produces heat and energy. Mitochondria have the biology and morphology of a bacterium and reproduce by fission. 13 During efforts, mitochondria reproduce, depending on the heart and muscles' energy intensity.14 During pregnancy, the heart's energy need increases exponentially, so mitochondria are stimulated by estrogens to reproduce to meet energy needs. Estrogen receptors alpha and beta are found on the membranes of mitochondria, suggesting the importance of this hormone in heat and energy production. 15 It is logical to assume that the heart during pregnancy requires enormous energy to increase cardiac output by a third.
The pathophysiology of the heart in postmenopausal
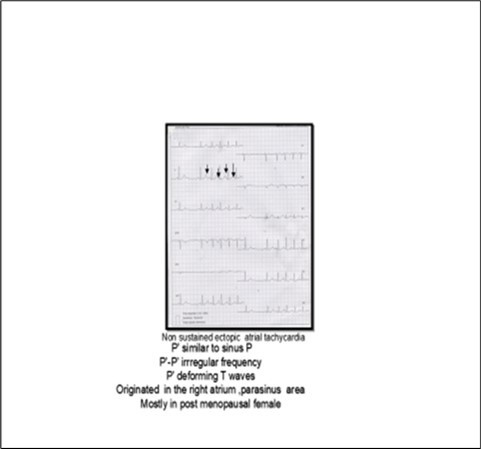
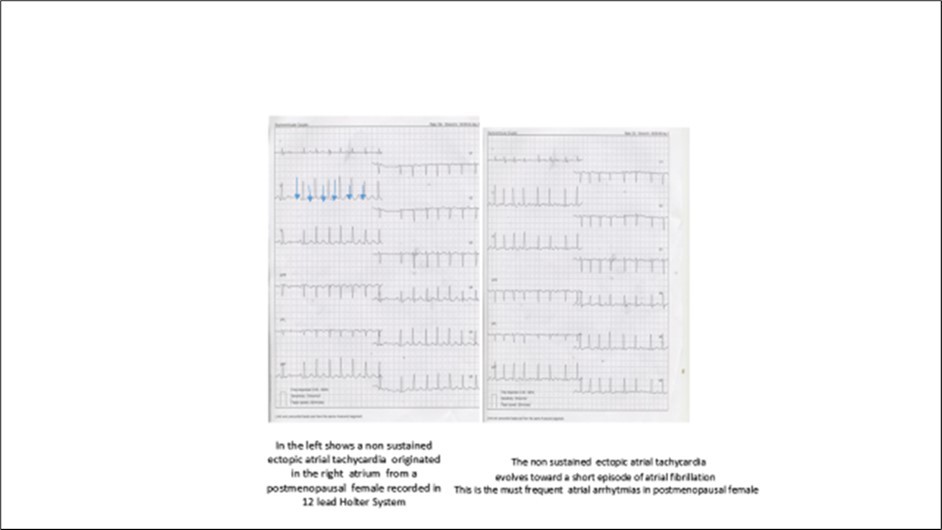
Inhypoestrogenemia, the fibroblast produces more collagen I than III,16 in the subendocardium of the left ventricle, and in the right atrium. From collagen I, fibrosis forms. 17This subendocardial fibrosis complicates diastolic relaxation. (12Increasing the heart rate increases the final diastolic pressure. (Figure 1) This hemodynamic phenomenon is reflected in dyspnea on effort, and in the case of very high frequencies, such as atrial fibrillation, can cause acute heart failure with normal cardiac contraction. In the right atrium, the fibroblast secretes collagen I , resulting in atrial fibrosis. The fibrotic right atrium is the basis for arrhythmias; And non-sustained ectopic atrial tachycardia,( Figure 2) which can evolve into limited atrial fibrillation.( Figure 3)The diastolic function is altered by the dysfunction of hypoestrogenemia in calcium metabolism.18 In the reduction of estrogen , the calsificvation of mitral annulus, aortic valve and, coronary arteries19
Figure 1.Sclarovky S and Heartz I 1994 Assuta Medical Center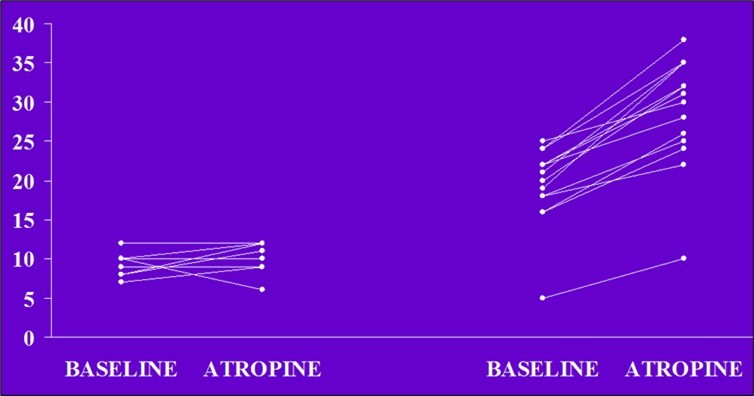
Estrogen has a critical function in the pump, SERCA, and phospholamban in transporting calcium to the sarcoplasmic reticulum. Therefore, this phenomenon contributes to diastolic dysfunction and an increase in final diastolic pressure 19 (Figure 1)
In extreme emotional situations, with high secretion of adrenergic substances, the myocardium is exposed to severe injuries, and due to the lack of estrogen control, it causes severe dyskinesia, which can trigger mortality. This phenomenon is called tako-tsubo, 20 occurring in 99% of women and 95% in postmenopausal women.
It is also logical to speculate that the heart of the postmenopausal woman has less cardiac energy due to hypoestrogenemia and the hormone's stimulating effect on alpha and beta receptors in the mitochondria's membrane.
Left side
5 wamen 30 to 49 years old
With angina pains
ECG inverted T waves in precordial leads
Cardiac ultrasound normal
Coronariography normal
Left diastolic pressure normal
After atropine no changes in intracavitary pressure
Intracavitary pressure suggesting severe diastolic failure
right side
10 postmenopausal wamen
with angina pains and dyspnea
with STdepression in v4.v5.v6
ultrasound signs of diastolic dysfuntion
coronariography normal
high diastolic pressure at rest
after atropine marked increase in I
References
- 1.Booz W, Baker K M. (1995) Molecular signaling mechanism controlling growth and function of cardiac fibroblat ;. , Cardiovas Res
- 2.Caudfield J B, Benjamini K S. (1997) structureand functionof myocardial fibrillar collagen ;Techn healt care;5;95-113 a.
- 3.Kramer E, Mahmodzale S, Schrier E. (2019) bh fibroblst sec collagen sex –specific regulacionon of collagen I and III expression by17 beta estradiol in cardiac fibroblat; role of estrogen receptor Cardiovac Reach;115;315-27.
- 4.Elkajan V OuzouminianJG. (2012) Phsiological changes during normal pregnancyand delivery;. , Cardiologic 30-317.
- 5.Grammer J B, Dofour A. (2005) atrial fibrosis in heart surgery patient decrease collagen III/Iratioin post operative atrial fibrillation ; basic ResCardiology;100;288-94.
- 6.Canberg K A, Fregly M S. (1986) Catecholamine excreationanda adrenergic responsiveveness in estrogen treated rats ;. 32-147.
- 7.Sato S, Kato N, al Kundey RK et. (1997) beta adrenergic receptors in stunned myocardium in consensius pigs J of molecular cell cardiology ;29;1387-400Botnik P.
- 8.Bonnely E, Avbin J E. (2002) differentiale expression of estrogen receptors- related receptors alfa and betain osteoblastoin vivo and vitro l Bone. 17, 400.
- 9.Butrago C, Masheme R, Boland A R. (2000) acute, modulationofcalcio influx in rats by beta estradiol’ Cell Signal. 12-47.
- 10.Bupha T, Watranapaperrmpoll J. (2006) regulatory role of ovarium in calcium uptake activityin sarcoplastic reticulum;. , J of Am of Physiolog
- 11.Botnik P, Unkel C. (1999) Regiona lexpressionof phosphanban in the human heart Cardiovac. Resh;43 67-76.
- 12.S Watanaspa CH Punphong, Wattaperpol J. (2015) Significantrole ofestrogenin maintaningcadiac mitochondrial function. , The J of Steroid and Biochemestry Molecular Biology 147-1.
- 13.Szinizuk K B, Srewezu M, K M. (2000) The similartgies betweenhuman mitocindrial and bacterias in the context structural genome ;Molecules. 25-2857.
- 14.Christiopher J. (2000) Mitocondrial plasticity in classical ischemic preconditioning , beyond mitocondril KATP channels Circ Res. 87.
- 15.Duckles S P, Krause D N, Stirone C H. (2006) Estrogen and mitochondria ;a new paradigm for vascular proteccion ;Intervention ;6;. 26-35.
- 16.N E Parotte, Alfrbi GM BidermanD. (2018) iMaternal cardiac messenger Expressionof intracellular matrix protein in in mice during pregnancyhe postpartum period Exp Biol Med ;243;. 1220-32.
- 17.Maslov P Z, Kim L K. (2019) A rguliane et al. , J of American cardiological college Heart failure 7-192.
- 18.Zao Z, Wong H, Jesgup J. (2014) . Role of estrogen in diastolic dysfunction ;Am J of physiology ; 306 , H628-H40 .